SMALLPOX
AND BIOLOGICAL WARFARE
The
first biological weapon
 Smallpox has the distinction of being
the first biological agent used against an enemy in war times. During the French and Indian war
(1754-1763), Lord Jeffrey Amherst served as commanding general of the British
forces, leading the British to victory against the French. The Ottawa Indians’ continued
Smallpox has the distinction of being
the first biological agent used against an enemy in war times. During the French and Indian war
(1754-1763), Lord Jeffrey Amherst served as commanding general of the British
forces, leading the British to victory against the French. The Ottawa Indians’ continued 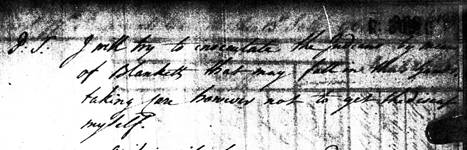 hostilities toward the British led to
the measures suggested by Colonel Henry Bouquet in 1763 to “try to inoculate
the Indians by means of blankets that may fall in their hands, taking care
however not to get the disease myself.”
Amherst officially
hostilities toward the British led to
the measures suggested by Colonel Henry Bouquet in 1763 to “try to inoculate
the Indians by means of blankets that may fall in their hands, taking care
however not to get the disease myself.”
Amherst officially 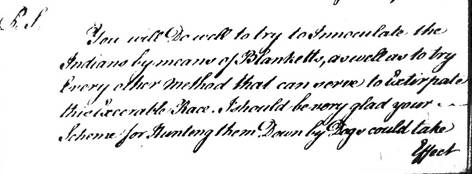 approved the strategy, replying in a
letter to Bouquet, “You will do well to try to inoculate the Indians by means
of blankets, as well as to try every other method that can serve to extirpate
this execrable race.” There were reports
of a smallpox epidemic the following spring among the Indians after blankets
and handkerchiefs were distributed to them at Fort Pitt (http://www.nativeweb.org/pages/legal/amherst/lord_jeff.html).
approved the strategy, replying in a
letter to Bouquet, “You will do well to try to inoculate the Indians by means
of blankets, as well as to try every other method that can serve to extirpate
this execrable race.” There were reports
of a smallpox epidemic the following spring among the Indians after blankets
and handkerchiefs were distributed to them at Fort Pitt (http://www.nativeweb.org/pages/legal/amherst/lord_jeff.html).
A modern threat
 Much of the literature in recent years
speaks of smallpox in the past tense.
With the eradication of the disease in 1980, and variola virus research
stocks restricted to two labs, the CDC and a lab in Koltsovo, Russia, no one
imagined that smallpox would again pose a threat to humanity. However, Henderson et al. (1999) report that
since that time a former Soviet bioweapons program deputy director revealed
that in 1980 the Soviets undertook a program to weaponize smallpox for use in
missiles. They were successful in this
endeavor, and because of the economic crisis in Russia, there are
reasons to fear that the technology could be bought by others seeking to commit
acts of terror.
Much of the literature in recent years
speaks of smallpox in the past tense.
With the eradication of the disease in 1980, and variola virus research
stocks restricted to two labs, the CDC and a lab in Koltsovo, Russia, no one
imagined that smallpox would again pose a threat to humanity. However, Henderson et al. (1999) report that
since that time a former Soviet bioweapons program deputy director revealed
that in 1980 the Soviets undertook a program to weaponize smallpox for use in
missiles. They were successful in this
endeavor, and because of the economic crisis in Russia, there are
reasons to fear that the technology could be bought by others seeking to commit
acts of terror.
The events of September 11, 2001, have heightened this fear. Since the smallpox vaccination program was
discontinued after eradication of the disease, much of the population is now
vulnerable to infection. Only laboratory
workers have continued to receive vaccinations, since the risks associated with
the vaccine were deemed unacceptable for the general public. Furthermore, vaccination does not provide
lifetime immunity; protection beyond 10 years is questionable, according to the
WHO.
Apprehension
about potential use of smallpox as a bioweapon led to concerns about the amount
of vaccine available. In early 2002 the
CDC undertook a study to test their vaccine stocks for effectiveness after
dilution. Our labs, which work with
vaccinia virus, were included in this study.
A few of us had received the vaccine prior to eradication, and a
subsequent “booster” in 1989 since we handle live vaccinia. However, since vaccination was not mandatory,
none of the young graduate students had ever received the vaccine. The diluted vaccines administered were all
successful, as evidenced by the various vaccination site lesions we endured,
and no one experienced any adverse reactions.
Results of this study indicate that a 1:10 dilution of the
vaccine retains its efficacy. Frey et
al. (2002), in a larger study, report comparable success rates (97.1 to 99.2%)
using 1:5 and 1:10 dilutions of
the vaccine.

Since those
studies, additional measures have been implemented to protect certain segments
of the population in the event of terrorism.
On December 13,
2002, President Bush announced that volunteer Smallpox Response
Teams would be formed to care for citizens should a smallpox attack occur. Team members, along with health care workers,
military personnel, and certain other civilians at risk would receive
vaccinations. At that time it was also
announced that there is now enough vaccine in the United States to vaccinate
all of its citizens. However, the future
of smallpox as a biological weapon – and as a disease we must once again
confront in the population - remains to be seen.
Addendum: On March
25, 2003, the CDC issued a statement recommending that people with a
history of heart disease should not be vaccinated against smallpox at this
time. This came in the wake of several
cases of heart problems after vaccine administration. Two of these resulted in death. Dr.Julie Gerberding, CDC director, in
discussing the safety of the vaccine, said, "We promised to closely
monitor this program and to put safety first, so we are exercising exceptional
caution. If our investigation shows this
precautionary measure should become permanent or the need for other changes or
enhancement in the civilian smallpox vaccination program, we will take
immediate action. We continue to believe
that it is important and necessary to vaccinate health care workers to prepare
our nation in the event we have to respond to a smallpox outbreak.”
 Return home
Return home